The term Non-Hodgkin’s lymphoma (NHL) describes a large group of lymphocyte malignancies. Bone marrow transplantation is a procedure more commonly used to treat leukemia than lymphoma. However, bone marrow transplant for non-Hodgkin’s lymphoma can be beneficial to some patients.
What is Non-Hodgkin’s Lymphoma ?
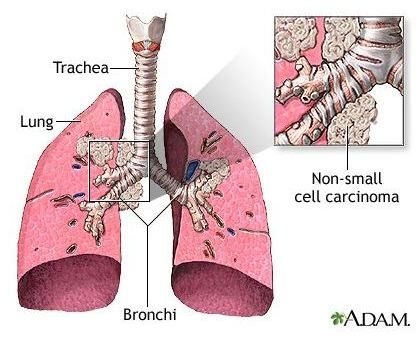
Lymphoma is a type cancer that arises in lymphocytes (white blood cells). Mutated lymphocytes proliferate uncontrollably, replacing healthy tissue and forming tumors. NHL account for around 90% of all diagnosed lymphomas. There are 35 different types of non-Hodgkin’s lymphoma. NHL usually appears as a solid tumour in the lymph nodes, usually in the neck, chest, armpit or groin but it can affect any lymph node or related tissue in the body.
NHL is a life-threatening, but improved treatments have caused the death rate to fall.
Treatment for NHL
There are several established treatments for NHL, most commonly chemotherapy. If the lymphoma is localized to one are of the body, radiatiotherapy might be used in combination with chemotherapy. In some types of advanced NHL, bone marrow transplant (BMT) or peripheral blood stem cell transplants (PBSCT) maybe used, particularly in cases that are not curable with chemotherapy alone.
High dose chemotherapy required to kill malignant cells, will also kill healthy bone marrow. Bone marrow is the living tissue within the bones which generates mature red cells, white cells and platelets. Therefore bone marrow damage leaves the patient with severely reduced immunity and vulnerable to infection, anemia and bleeding. Therefore new cells are transplanted in order to repopulate the bone marrow and restore immunocompetance.
Bone Marrow Transplant for Non Hodgkin’s Lymphoma
HSCT are more commonly performed than BMT, but a bone marrow transplant may be carried out if collection of stem cells proves difficult. Bone marrow transplant for non-Hodgkin’s lymphoma is most commonly performed if:
- the chance of relapse is considered to be high
- the patient has relapsed
- the patients has not responded to other treatments
BMT or HSCT are described as autologous or allogeneic, depending on the source of cells:
- Autologous BMT: a sample of the patients bone marrow is harvested are stored prior to the start of chemotherapy.
- Allogenic BMT: bone marrow is collected from a healthy donor, usually a sibling.
Bone marrow collected by passing a needle through the hip bone and/or chest bone whilst under general anaesthetic. Blood transfusion and pain killers are often necessary after the procedure. After the course of chemotherapy has finished the bone marrow is infused into the patient through a drip. After entering the bloodstream, the stem cells travel to the bone marrow, where they begin to produce new white blood cells, red blood cells and platelets; a process called engraftment. This usually occurs within 2-4 weeks and can be monitored by regular blood tests. Complete recovery of immune function can take several months or even years however.
Bone Marrow Transplant Risks
Patients may suffer short-term side effects such as nausea, vomiting, fatigue, loss of appetite, mouth sores, hair loss and skin reactions after BMT or PBSCT .
In allogeneic transplants, a complication known as graft-versus-host disease (GVHD) can occur. White blood cells from the donor recognise cells in the patient as ‘foreign’ and attack them. This most commonly involves the skin, liver and intestine. Immunosuppressive agents can be used to prevent or treat this complication.
References
Cancer Research UK www.cancerhelp.org.uk
Leukaemia Lymphoma Research www.beatbloodcancers.org
National Cancer Institute www.cancer.gov