How would physicians have coronary heart disease explained to their patients. Learn the basics of the disease in this overview.
About Coronary Heart Disease
Coronary heart disease (CHD) is the leading cause of death in the United States. Also known as coronary artery disease (CAD), it occurs when the arteries that supply the heart muscle with oxygen-rich blood become blocked or narrowed. Some individuals are at greater risk of developing CHD, and patients with increased risks should schedule regular appointments with their doctors. There are several aspects to understand in order to have coronary heart disease explained.
Causes
There is really only one underlying cause of coronary heart disease, and the disease process is life-long in most patients. Beginning during adolescence, the walls of arteries, especially those of the heart, become streaked with fatty plaques. This is the beginning of a process called atherosclerosis. As atherosclerosis progresses, these fatty streaks begin to collect circulating collagen, lipids, cholesterol, cellular wastes and fibrin, which is a circulating protein that helps blood clot during trauma. All of these materials cause the plaque to grow, and the circumference of the artery to shrink. As the artery narrows, the likelihood of a cardiac incident increases.
Risk Factors
There are several risk factors that affect the likelihood of disease progression. Cigarette smokers carry a high risk of coronary heart disease; pipe and cigar smokers have a slightly smaller risk, but still more so than nonsmokers. Smoking increases the speed of plaque growth in arteries. High levels of low-density lipoproteins (LDLs) and triglycerides coupled with low levels of high-density lipoproteins (HDLs) increase a patient’s risk. As does high blood pressure levels (hypertension). Patients with these conditions are often overweight or obese and exhibit inappropriately low levels of activity. All of these are controllable or “modifiable” risk factors.
Other risk factors are uncontrollable or “unmodifiable”. These include advanced age; approximately 85 percent of patients who die of CHD are 65 years of age or older. Family history of CHD puts patients at an increased risk. African Americans, Hispanics, native Hawaiians and some Asian American patients are in high-risk populations, over which they have no control. Male patients have higher risk than females; however, post-menopausal women’s risk increases but is still not as high as men’s.
Symptoms
The disease progresses slowly in many patients. Therefore, many patients do not experience symptoms until middle or late age. When symptoms appear, they often take the form of chest pain, called angina pectoris. This pain may radiate out from the chest to the arms, neck or abdomen. Often this occurs during increased oxygen-requiring states, such as exercise or emotional stress. Some patients experience numbness in the extremities. Shortness of breath (SOB) may also present, as well as being easily fatigued. Patients who experience a lack of blood to the heart muscle (cardiac ischemia) without pain are said to have experienced silent ischemia.
Complications
The complications of coronary heart disease can be fatal, or at the very least, may impair the way your heart functions permanently. If ischemia to the heart muscle occurs, patients may suffer a myocardial infarction (MI), or heart attack. If treatment is delayed, damage to the affected heart muscle may occur. If this occurs chronically, the muscle may become too weak to meet the body’s needs and heart failure occurs. Should a blood clot form at the site of an atherosclerotic plaque and block the blood supply to the brain, a cerebrovascular accident (CVA), or stroke, may occur. Also impaired blood flow to the heart may affect its normal electrical rhythm, causing an abnormal heart rhythm (arrhythmia).
Diagnosis
Physicians perform several tests to diagnose CHD, usually after a determination of high risk. Generally an electrocardiogram (EKG or ECG) and an exercise stress test will be performed. Physicians will do blood work to determine levels of certain substances. If required, invasive testing may be necessary, such as cardiac catheterization in order to get a picture of problem areas. Other diagnostic tests may include nuclear imaging, echocardiograms and X-rays.
Management and Treatment
The first step to disease management is prevention. This includes leading a healthy lifestyle by maintaining a proper weight, getting regular exercise, eating a healthy diet and not smoking, or at least quitting. If you are diagnosed with coronary heart disease, lifestyle changes are necessary to slow disease progression. Your physician will attempt to control the disease with certain medications, which must be taken regularly. Medications include cholesterol modifiers, aspirin, beta blockers, nitroglycerin, calcium channel blockers and angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs).
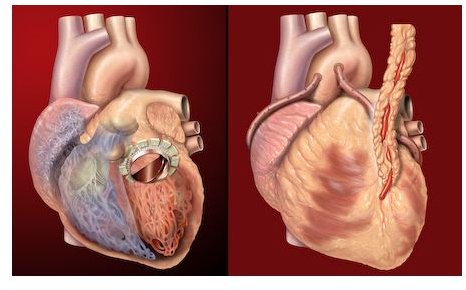
If necessary, doctors may suggest invasive surgery to correct the problem. Fortunately, many current procedures are minimally-invasive. Learn more about some of the procedures used in the treatment of vascular diseases and coronary artery bypass grafting (CABG) .
References
Cleveland Clinic: Coronary Artery Disease Overviews
Mayo Clinic: Coronary Artery Disease
MedlinePlus Medical Encyclopedia: Coronary Heart Disease
Texas Heart Institute: Coronary Artery Disease
Columbia University Department of Surgery: Cardiac, Coronary Artery Disease
American Heart Association: Atherosclerosis
American Heart Association: Risk Factors and Coronary Heart Disease